Shock and awe: the role of ESWT in healing athletes

Extracorporeal shockwave treatment (ESWT) was developed over 40 years ago to disintegrate urinary stones. Over the last 25 years, it has evolved into a treatment for musculoskeletal injuries. Whereas the original shockwave devices were used to disintegrate tissues, orthopaedic ESWT therapy causes regeneration in tissue. This therapy ellicits a number of biological responses at the molecular, cellular and tissue levels, which impact the management of certain sporting injuries. The diagnoses which benefit from ESWT include the following(1,2):
- Plantar fasciitis
- Lateral elbow epicondylitis.
- Calcific tendinopathies of the shoulder
- Patellar tendinopathy
- Achilles tendinopathy
- Adhesive capsulitis (frozen shoulder – see this article)
- Non-union of long bone fractures
- Avascular necrosis of the femoral head
- Greater trochanteric pain syndrome
- Medial tibial stress syndrome
- Proximal hamstring tendinopathy
ESWT technology
There are essentially two types of shockwaves produced(3):- Focused ESWT (F-ESWT)
- Radial Pressure Waves (RPW) - also known as radial shockwaves
Although they share certain similar characteristics, they are different in terms of how the wave is generated, the actual properties of the wave and the way the wave works on the cells and tissues. Similar to therapeutic ultrasound, ESWT uses sound waves to induce change in tissues. However, the pattern of the acoustic wave in ESWT is uni-phasic (whereas ultrasound is bi-phasic) with peak pressures as high as 500 bars, which can be 1000 times greater than ultrasound waves -thus producing a more potent therapeutic effect(1). The generated ESWT sound pressure waves may be focused or radial in nature (see panel 1 ).
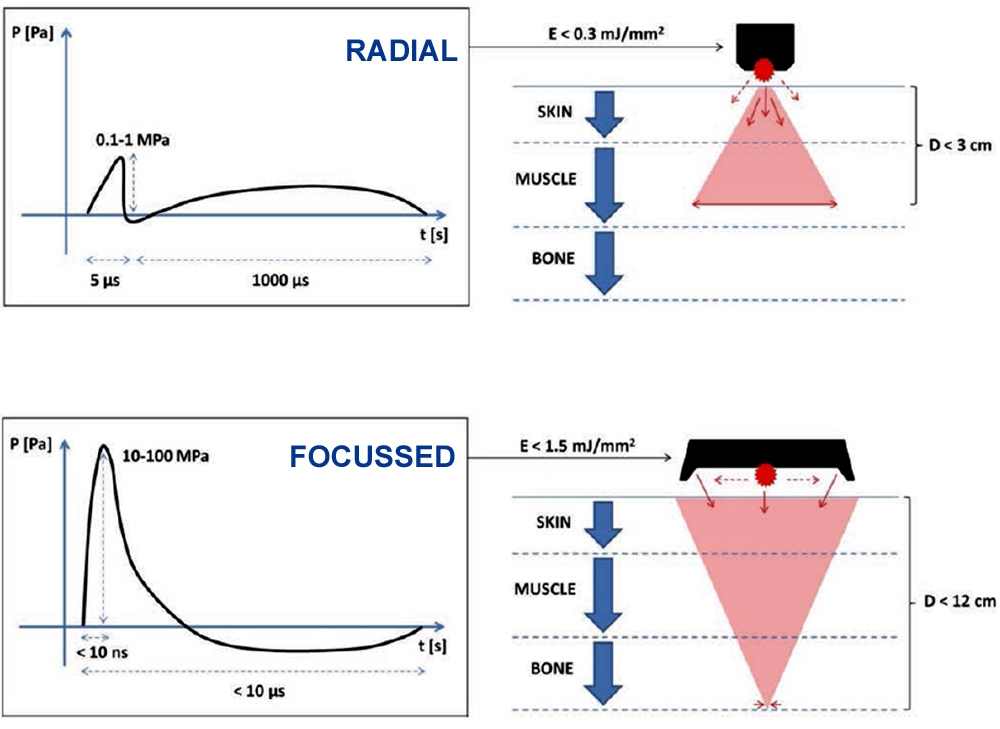
Panel 1: Focused vs. radial pressure waves in ESWT
*Focused ESWT- In focused ESWT (F-ESWT), the shockwave is produced by using an electrohydraulic source (such as a spark plug), an electromagnetic source (such as coils), or a piezoelectric source. These methods can generate a wave that is reflected (via an ellipsoidal or parabolic reflector) and then concentrated onto a focus point(3). This type of shockwave is particularly effective for tissues deep inside the body (up to 12cm -see figure 1). However, although this type of treatment is gaining popularity, the cost of the device to produce focused waves prohibits the use of this in most private clinical settings. Furthermore, because the use of F-ESWT requires high energy, it necessitates accurate identification of the focus area to be treated, via the use of radiologic or ultrasound guidance(1). This is very difficult to achieve in clinical settings.*Radial ESWT - Radial shockwave (RPW) generators work by compressing air, which then accelerates a projectile in a guiding tube. The result is a wave that is radially expanded as it leaves the tube and into the tissue. This does not produce a shockwaves as such but instead creates acoustic cavitation As a result, the penetration depth is not great (less than 3cm). These are best used on wide areas of the body; the energy produced by the pressure wave is highest at the skin surface, diverging and weakening as it penetrates deeper. This is a more cost effective option and is the more common type used by therapists treating in private practice.
In summary, the key differences between these types of therapeutic waves are pressure distribution, energy density and total energy at the focal point - measured as the ‘energy flux density’ in mJ/mm² per impulse(4).
Figure 1: Radial versus focused shockwave patterns
Mechanism of action
ESWT conducts a mechanical stimulus via pulsed acoustic waves, enhancing tissue regeneration by converting the stimulus into biochemical signals through ‘mechanotransduction’(5). There are four proposed mechanisms of action of ESWT(6,7):- Physical - The pressure of the wave imparts physical energy to the tissues in the form of absorption, reflection, refraction, and transmission(8). Furthermore, the stimulus creates a tensile force, which produces cavitation in the tissue. This increases cell membrane permeability and ionization of the molecules, which help activate signal transduction pathways(9-11).
- Physiochemical - The stimulus alters ion channel functions, thus stimulating cells to release substances such as ATP to activate cell signal pathways(12), and to mobilize calcium movement within cells(13).
- Biological - Through activating the secretion of a host of growth factors, such as angiogenesis, nitric oxide synthesis, and insulin-like growth factors(13).
Another theory is that ESWT works by altering the transmission of pain stimuli and thus increases a patient’s pain tolerance. This decrease in pain sensation occurs by activating small diameter fibers that then trigger the serotoninergic system(14). The overall effect of the four aspects of ESWT is to promote chondroprotection, neovascularisation and neoangiogenesis, tenocyte and fibroblast proliferation, collagen deposition, and to subsequently enhance tissue remodeling (15). The use of EWST appears to also decrease inflammation(16).
Clinical indications
The research summaries below outline the effectiveness of ESWT in a variety of musculoskeletal conditions (see also table 1).*Calcific tendinopathies of the shoulder
High energy ESWT in calcific shoulder tendons results in pain improvement, and improved function and calcium resorption in 71-88% of cases(17-20). By contrast, low energy ESWT is less effective, benefiting only 37% of cases(18).
*Noncalcific tendinopathies of the shoulder
There is no strong evidence for the use of ESWT in the non-calcific versions of shoulder tendinopathy (ie typical tendon degeneration conditions and tears that do not have a calcific pathology)(3,21).
*Tennis elbow (lateral epicondylitis)
Some authors have found improvements in pain and function with the use of F-EWST and RPW compared to placebo groups, although the data is limited(22,23).
*Greater trochanteric pain syndrome
Some studies have shown favorable outcomes in lateral hip pain after a quite long treatment period (four months), and more positive benefits in the medium to long term compared with home exercise and steroid injection(24,25).
*Patellar tendinopathy
Current evidence supports the use of F-ESWTand RPW for patellar tendinopathy with moderate or low-intensity protocols, especially in patients attempting to avoid an invasive intervention(26).
*Achilles tendinopathy
When combined with eccentric loading, the use of low-energy ESWT has shown to be effective in improving pain and function in both insertional and non-insertional tendinopathy(27).
*Plantar fasciitis
The American College of Foot and Ankle Surgeons Group has recommended ESWT as the treatment of choice for plantar fasciitis, with or without a plantar spur, when non-operative treatment has failed(28).
*Adhesive capsulitis of the shoulder (frozen shoulder)
Studies into the use of ESWT on adhesive capsulitis versus conventional physiotherapy (heat packs, ultrasound and interference current therapy) showed that while both groups experienced improvements at the end of the four weeks of treatment, the ESWT group had a lower level of pain and a higher range of motion than the therapy group(29). As mentioned above, readers are referred to a recent Sports Injury Bulletin article by Andrew Hamilton, which covers the use of ESWT (along with a number of other therapies) in the treatment of adhesive capsulitis.
*Bone Disorders
The use of ESWT on bone lesions is thought to stimulate bone healing by upregulating and expressing pro-angiogenic and pro-osteogenic growth factors(9). Strong evidence from numerous studies suggests that ESWT is effective for delayed union and non-union of fractures(3).
| Pathology | Technology | Grade of recommendation |
|---|---|---|
| Calcific Tendinopathy of the shoulder | F-ESWT | Good level of evidence |
| Calcific Tendinopathy of the shoulder | RPW | Insufficient evidence |
| Non-calcific tendinopathy of the shoulder | F-ESWT or RPW | Poor level of evidence |
| Tennis elbow | F-ESWT or RPW | Fair level of evidence |
| Greater Trochanter Pain | PRW | Fair level of evidence |
| Patella tendinopathy | F-ESWT or RPW | Fair level of evidence |
| Achilles tendinopathy | F-ESWT or RPW | Fair level of evidence |
| Plantar fasciitis | F-ESWT or RPW | Good level of evidence |
| Bone nonunion | PRW | Fair level of evidence |
In summary
Extra corporeal shock wave therapy is a non-invasive treatment that uses the mechanical force of a powerful acoustic shock wave within injured tissues to reduce pain and speed healing of the affected area. On the balance of evidence, ESWT is effective in pain reduction and functional improvements in calcific pathologies of the shoulder and in plantar fasciitis. It may also have a fair degree of success in other types of musculoskeletal injuries such as Achilles/patella tendinopathies, tennis elbow, greater trochanteric pain, and bone malunions. Along with load management and rehabilitation interventions, ESWT may be an effective adjunct to treatment prior to invasive procedures such as injections and surgery.References
- Journal of Orthopaedic Surgery and Research 2012, 7:11
- Br J Sports Med 2018;52:387–407
- Moya J Bone Joint Surg Am. 2018;100:251-63
- Ultrasound Med Biol. 2012;38:1673–80
- Med Princ Pract 2014;23:7–13
- J Urol. 1997 Jul;158(1):4-11
- J Urol 1992, 39:529-32
- Clin Orthop Relat Res. 2001 Jun;387:8-17
- J Orthop Res. 2003 Nov;21(6):984-9
- Cardiovasc Res. 2016 Feb 1;109 (2):331-43
- 2014 Feb;37(1):65-70
- J Biol Chem. 2014 Sep 26;289(39):27090-104
- Muscles Ligaments Tendons J. 2012 Apr 1;1(4):138-47
- J Bone Joint Surg Br. 2004; 86(4): 613-618
- Muscles Ligaments Tendons J. 2012;2:33–7
- Eur J Phys Rehabil Med. 2014;50: 217–30
- Phys Ther. 2006 May;86(5):672-82
- 2003 Nov 19;290(19):2573-80
- Ann Rheum Dis. 2003 Mar;62(3):248-50
- J Shoulder Elbow Surg. 2008 Jan-Feb;17(1):55-9
- Man Ther. 2011 Oct;16 (5):419-33
- Int J Surg. 2015 Dec;24(Pt B):165- 70
- J Bone Joint Surg Am. 2005 Jun;87 (6):1297-304.
- Am J Sports Med. 2009 Oct;37(10):1981-90
- Am J Sports Med. 2009 Sep;37(9):1806-13
- Knee Surg Sports Traumatol Arthrosc. 2013 Feb;21 (2):346-50
- Foot Ankle Int. 2013 Jan;34 (1):33-41
- J Foot Ankle Surg. 2010 May-Jun;49(3)(Suppl):S1-19
- J Phys Ther Sci. 2017 Nov; 29(11): 1907–1909
You need to be logged in to continue reading.
Please register for limited access or take a 30-day risk-free trial of Sports Injury Bulletin to experience the full benefits of a subscription. TAKE A RISK-FREE TRIAL
TAKE A RISK-FREE TRIAL

Chris Mallac

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.