You are viewing 1 of your 1 free articles
Plyometric training…when does rehabilitation need a spring in its step?

‘Plyometric exercise’ was a term coined in 1964(1). Plyometrics exercises exploit the benefits of the plyometric regime and involve the Stretch-Shortening Cycle (SSC)(2). Thanks to the muscles’ pre-stimulation during the eccentric phase, plyometrics exercises are able produce high amounts of power(3). In a plyometrics exercise, muscles undergo contractions during three different ‘conditions’(4):
- ‘Miometric’– ‘mio’ is a Greek prefix meaning shorter.
- ‘Isometric’– ‘iso’ means same.
- ‘Pliometric’– ‘plio’ means longer.
The benefit of plyometric training is related to its capacity to improve the reactive ability of the neuro-muscular system, thus allowing greater force production in the concentric phase of SSC(5). This is achieved thanks to the following factors:
- Miogenic (Myogenic)– the utilization of the elastic energy storage in muscle-tendon tissue.
- Neurogenic– the alteration of the timing and firing rates of the motor units involved in myotatic reflex.
Myotatic Reflex
The myotatic reflex is a monosynaptic reflex which triggers the automatic contraction of muscles when their stretch receptors are stimulated (see figure 1)(5). When a muscle is stretched, Group 1a afferent neurons in the muscle spindle react to changes in muscle length and velocity. This activity transmits information to the spinal cord through changes in the rate of action potentials.Figure 1: Myomatic reflex mechanism*
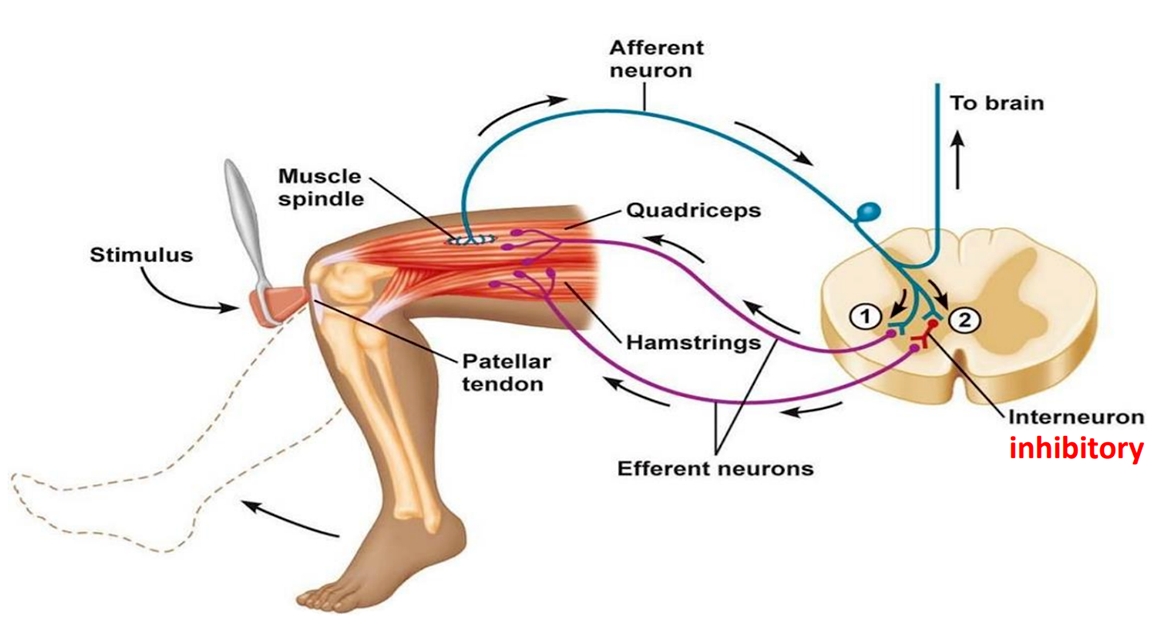
Myotatic Reflex involving the communication between the muscle's stretch receptors and spinal cord. NB: 1 = Somatic motor neuron efferent path. 2 = Interneuron inhibiting somatic motor neuron.
*Image courtesy of Laiche Djouhri, Dept. of Physiology, King Saud University
The 1a afferent signals are transported monosynaptically to alpha motor neurons at the spinal cord. Signals then pass from the motor neuron to the extrafusal fibers of the muscle via the efferent axons, thereby generating force and resistance of the initial stretch.
In coordination, the 1a afferent signals are also sent polysynaptically through interneurons in the spinal cord, called Renshaw cells. Renshaw cells are special inhibitory interneurons. They inhibit the alpha motor neurons of the antagonist muscles and cause it to relax. This relaxation is called reciprocal inhibition.
If the initial muscle stretch tension is too high, and there is a chance of fiber breakdown, a ‘sensor’ structure called the Golgi Tendon Organ (GTO) provides a contraction inhibition via 1b afferent fibers at spinal-cord level. The GTO is situated at the junction between the extrafusal muscle fibers and the tendon itself. It is attached to muscle fibers via collagen fibers(6).
The stretch-shortening cycle
Plyometric training utilises the SSC by using a lengthening movement (eccentric), which is quickly followed by a shortening movement (concentric) (see figure 2). The transition phase between the eccentric and concentric contraction is called the amoritization (isometric) phase(7). This phase is also referred to as ‘time to rebound’(7), and is measured as the ‘coupling time’(6).Figure 2: Phases of the stretch-shortening (SSC) cycle(8)
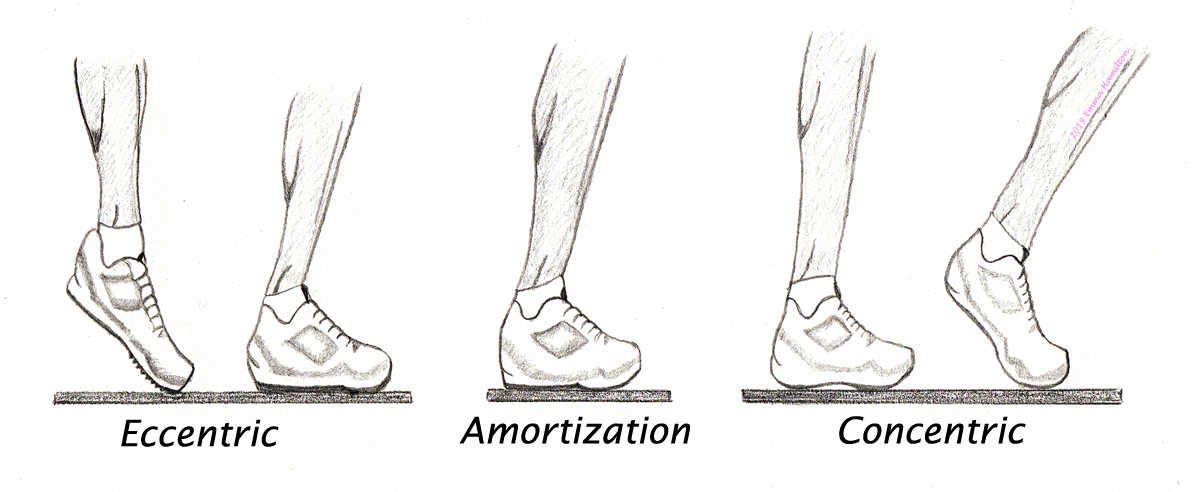 Eccentric pre-stretch phase occurs during landing or lowering. Amortization is the pause before the concentric phase which follows before the jump.
Eccentric pre-stretch phase occurs during landing or lowering. Amortization is the pause before the concentric phase which follows before the jump. *Eccentric pre-stretch phase
This phase of plyometric activity stretches the muscle spindle as well as the non-contractile or passive tissues within the muscle. These non-contractile tissues include the series elastic components (SEC) and parallel elastic components (PEC). the SECs consist of tendon tissue and myofilaments while the muscle sheath and sarcolemmas are considered PECs. The potential kinetic energy is stored in the SEC(7,9). The muscle’s elastic components have a major impact on force production(9). Seventy two percent of the elastic energy regeneration comes from tendon tissue, whereas 28% comes from contractile elements of the muscle(10).
*Amortization phase
This phase is the time delay between overcoming the negative work of the eccentric pre-stretch and generating force production and accelerating muscle contraction (due to elastic recoil)(7). The shorter this phase, the more powerful the plyometric movement because the more efficiently the stored energy is used during the transition. If this phase is delayed and coupling time is elongated, the stored energy is wasted as heat, and the stretch reflex is not activated(5).
*Concentric phase
Force production is created using the elastic recoil of the elastic - PEC and SEC - tissues(7). The magnitude of the elastic recoil will depend on the size of the external force that is trying to stretch the muscle(9). The SEC accounts for 70-75% of the concentric force increases(7).
Physiological benefits of plyometrics
The myogenic and neurogenic benefits of plyometrics exercises include(5-7):- Effective neuromuscular stimulation and improved intramuscular coordination between fibers to synchronize a higher recruitment of motor units.
- Elevated Renshaw cells’ inhibition threshold, enabling higher frequency of activation.
- Decreased GTO sensitivity to allow maximum concentric contraction.
- Greater elastic energy storage, which therefore creates faster contraction and improves neuromuscular spindles’ efficiency.
- Reinforced tendon, aponeuroses, and muscle connective tissues.
- More efficient reaction of mechanoreceptor stimulation in the joint capsule and ligaments.
These physiological benefits can produce the following training benefits(7,11):
- Ability to increase average power and velocity.
- Increased peak force and velocity of acceleration.
- Increased time for force development.
- Improved energy storage in the SEC.
- Increased tolerance of workloads without the GTO firing.
- Linked to decreased risk of re-injury.
Interestingly, the increase in performance often occurs without a corresponding increase in morphological changes in the muscle. Training effects of the neural system dominate the first 6-8 weeks of training. Hypertrophic changes in the muscle begin to occur following several additional weeks of training(7).
Criteria for implementation
Implementing plyometric training into rehabilitation should be contextual and individualized to the participant(11). The following factors should be considered(7,12):- Age (of the participant)
- Injury history
- Type and site of injury
- Medical history and health/condition
- Appropriate prior warm-up
Another important consideration is the participant’s level of foundational strength and their resistance training experience(7,13). Greater muscular strength can enhance the force-time characteristics (ie rate of force development and external mechanical power) of an individual, and is strongly correlated to superior jumping, sprinting, change of direction, and sport-specific performance(13,14). A structured and individualized resistance-training program is therefore recommended - preceding and alongside plyometric training - and integrated into the totality of the rehabilitation.
Plyometric training should be as specific to the patient’s performance demands as possible, and should be a bridge between rehabilitation and sport specific activities(7). In addition to an adequate base level of strength, the participant should ideally have full range of movement in the injured area, as well as measurable improvements in neuromuscular control, using objective markers such as the Y-balance single-leg squat, and 30-second single-leg balance tests(7). The athlete should be pain-free in weight bearing.
How to implement lower limb plyometric training
A plyometric program should follow the principles of progression and overload(6-9,13-15). This can be achieved by manipulating the volume dosage of different variables (eg repetitions, sets, weight, height, distance, etc)(7). The intensity of the work should be performed at high levels of intensity (80-100% maximum volitional contraction) in order to recruit fast twitch IIa and IIb fibres(7,8).Exercises are often performed through jumping, bounding, and hopping. Before initiating higher level jump training, lower level plyometric activities can be used to test the participant’s tolerance. The figures below provide examples of how to progress plyometric activities, starting with ‘beginner’ exercises and progressing through ‘advanced’ in relation to training stress(7).
Examples of progression of lower limb plyometric activities(7,15)



Squat Jump


Box Jump



Depth or Drop Jump



Drop Jump onto Second Box
In plyometrics, the volume of exercise is regulated through foot contacts. Below are recommended foot contacts per session for various levels of athletic ability(15):
- Beginner: 80-100
- Intermediate: 100-120
- Advanced: 120-140
There is limited research on optimum recovery times, but 48-72 hours between training bouts is generally recommended(7).
References
- Wilt, F. (1964). Track Technique. 64: 2024-2054
- Komi, P.V. (2003). Strength and Power in Sport. Blackwell Publishing
- Faulkner, J.A. (2003). J Applied Physiol. 95: 455-459
- Hubbard, A.W. & Stetson, R.H. (1938). J Physiol. 124: 300-313
- Bosco, C. & Rusko, H. (1983). Acta Physiol Scand. 119(3): 219-224
- Verkhoshansky, N. (2012). Central VA Sport Performance Seminar.
- G. et al (2015). Int J Sports Phys Th. 10(6): 760-785
- Radcliffe, J. & Farentinos, R.C. (2009). High Powered Plyometrics. Human Kinetics
- Bosch, F. (2015). Strength Training and Coordination: An integrative approach. 2010 Publishers
- Bisciotti, G. N. et al (2000). Med Del Sporto. 53(2): 125-135
- Mendiguchia, J. et al (2017). Med Sci Sports Exerc. 49(7): 1482-1492
- Jeffreys, I. (2007). J UKSCA. 6: 12-18
- Suchomel, T.J. et al (2016). Sports Med. 1-31
- Spiteri, T. et al (2014). J S&C research. 28(9): 2415-2423.
- Chmielewski, T.L. et al (2006). J Orthop Sports Phys Ther. 36(5): 308-319
Patrick Gillham

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.