You are viewing 1 of your 1 free articles
Pellegrini-Steida syndrome – a cause of stubborn medial knee pain

Calcification of soft tissue structures is not uncommon in the body. This process frequently occurs in the shoulder, with the supraspinatus tendon being the most commonly affected. After the shoulder, the hip is the second most frequent location followed by the elbow, wrist, hand, and the ankle/foot(1). In the knee, calcification frequently occurs near osseous attachments of the ligaments or the popliteal tendon(1). An infrequent occurrence is calcification at the medial collateral ligament (MCL), particularly at the level of its femoral insertional area(2). Usually this presentation is asymptomatic; in a case of pain however, it is known Pellegrini-Steida Syndrome (PSS- see X-ray image in figure 1).
Figure 1: Calcification of the MCL leading to pain (Pellegrini-Steida Syndrome)
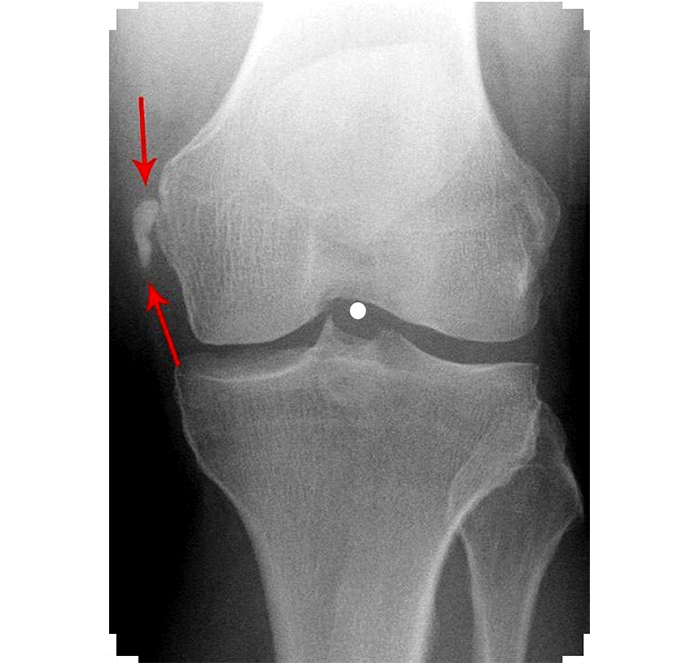
Calcified region indicated between red arrows
Why does calcification happen?
Calcified material is made up of calcium phosphate (otherwise known as calcium hydroxyapatite) crystals which are deposited into periarticular or intra-articular soft tissues, most commonly tendons. It is otherwise known as hydroxyapatite deposition disease and is included under the umbrella term pyrophosphate arthropathy(3). The aetiology of this process is still uncertain; however, the most common cause is believed to be owing to ‘dystrophic calcification’. This occurs as a reaction to tissue injury, which can be from isolated or repeated trauma over time(1).Injuries of the MCL
The MCL is the most commonly injured ligament in the knee(2,4). The majority of medial knee ligament tears are isolated and involve a valgus knee loading mechanism, as well as external rotation or a combined vector(5). Injuries are most common in athletes compared to non-athletes, especially in sports involving collision and contact-type trauma. Injuries in the sports-active population stands at around 7.3 injuries per 1000 athletes per year. Of those, 73% are grade I injuries, 23% grade II, and 4% grade III(2) (see table 1 below).
| Possible differential diagnosis | Exclusion criteria |
|---|---|
| Lumbar spine facet arthropathyDisc degenerationRadiculopathy | No diffuse leg referral+ve hamstring load testsLumbar palpation (NAD) & -ve quadrant test |
| Hip joint ischiofemoral impingement+/- Quadratus femoris abnormalities | Femoral external rotation in hip neutral -veMRI -ve (No loss of space and QF normal)Flexion-adduction-internal rotation (FADDIR) -ve |
| SIJ somatic referral | Lasletts’s SIJ provocation tests -ve |
| Sciatic nerve compression | Sciatic tenderness at QF -veSlump test +ve hamstring but no change with sensitisers (Hip adduction/internal rotation)Modified slump (lx extension) Differential test for specific comparison to PHT*Coexisting pathology possible |
| Deep gluteal syndrome/ Piriformis syndrome | Sciatic nerve non-tender at piriformisNo further provocation with piriformis stretch/contraction or slump with Add/IRMRI imaging -ve |
| Gluteal tendinopathy | +ve Hamstring load tests-ve gluteal load testsMRI -ve |
| Ischiogluteal bursitis | Pain with stretch and localised palpationIrritable symptoms with sittingMRI and ultrasound -ve |
| Partial or complete tear of the gluteal or hamstring muscle/tendon | Gluteal and hamstring tests +ve but MRI and U/S findings -ve for muscle or tendon tear respectively |
| Posterior pubic or ischial ramus stress fracture | Tenderness over ischial ramusMRI imaging -veHigh suspicion in female triad athletes |
| Adductor magnus pathology, tear or tendinopathy | Adductor tests -ve,PSST adductor stretch and resist -veMRI -ve |
| Vascular endofibrosis | No immediate resolution of symptoms on cessation of provocative exercise.Bruit sign -veEchography or arteriography -ve |
The structures of the medial knee are divided into the proximal and distal divisions. This consists of the superficial MCL (sMCL), the posterior oblique ligament (POL), and the deep MCL (dMCL) (see figure 2 below).
Figure 2: Structures of the medial knee*
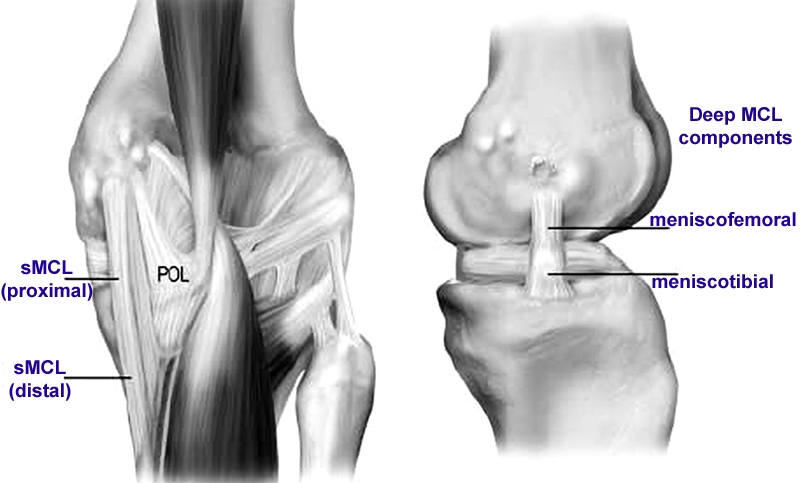
*adapted from J Bone Joint Surg (2007); 89(9)
The sMCL is the largest structure and consists of one femoral and two tibial attachments. The central arm of the POL is an extension off the distal aspect of the semimembranosus, which reinforces the posteromedial aspect of the joint capsule. The dMCL is divided into meniscofemoral and meniscotibial components, and comprises the thickened joint capsule deep to the sMCL(4).
The MCL has been shown to contribute 78% to the restraining force on the medial side of the knee. The sMCL has main control of valgus forces throughout the full range of movement, and helps to limit external rotation of the tibia when the knee is beyond 30˚of flexion. The dMCL mainly controls the anterior tibial translation of the flexed and externally rotated knee. Its role in controlling valgus stress is less relevant. The POL is tight in extension and in the first degrees of knee flexion. It controls posterior tibial translation as well as external rotation(2,4,5).
Presentation of PSS
PSS is most commonly developed in the tissue of the sMCL. In the majority of cases, this occurs following trauma to the MCL tissue. However, there have been cases without specific trauma(1,3). As a result, there is debate as to whether the calcification occurs in these cases due to hydroxylapatite deposition disease rather than trauma(3).According to literature, it takes around 2-6 weeks to develop post-traumatic calcific deposits(6). The deposition in the ligamentous tissue leads to inelasticity of the structure and generates pain. Athletes will complain of stiffness particularly when attempting to straighten the knee. Twisting activities will be aggravating, as well as impact-related exercise. Sensitivity of the medial knee to touch will be a common complaint, for example in positions when in contact with the other knee.
The patient can also present with mild swelling to the medial side of the knee, particularly close to the femoral attachment of the sMCL. There can be light warming to touch, but pain on palpation specifically. A palpable lump may also be present. Forced extension and flexion can provoke pain when examining. Ligamentous testing is stable when assessed, although valgus stress can produce pain especially with some external rotation added(2,5). This is particularly aggravating past 30˚of knee flexion, which is when the sMCL is more biased.
Awareness of adductor magnus or medial gastrocnemius involvement is important as a result of their proximity to the MCL structure (see figure 3 below)(7). Strength and length testing of these muscles is worth including in the assessment.
Figure 3: Proximity of adductor magnus and medial gastrocnemius tendon to sMCL
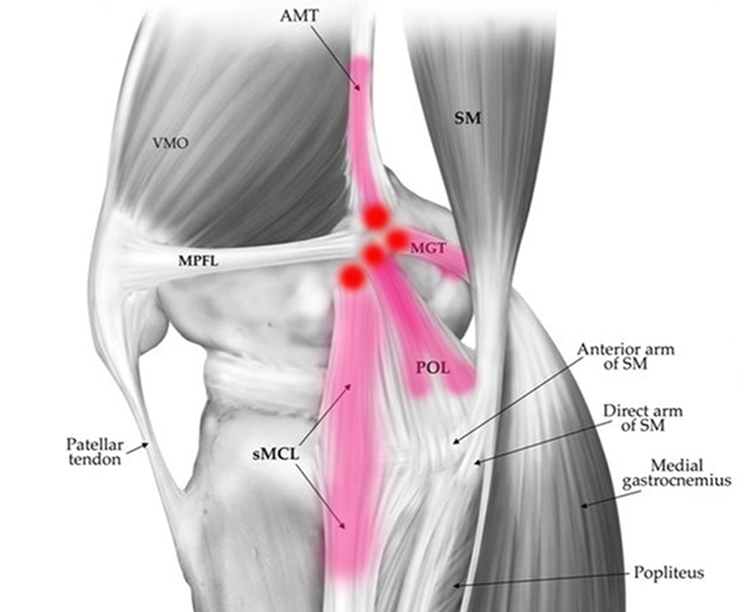
AMT=adductor magnus tendon, VMO=vastus medialis obliquus muscle, SM=semimembranosus muscle, MPFL=medial patellofemoral ligament, MGT=medial gastrocnemius tendon, ME=medial epicondyle, AT=adductor tubercle, and GT=gastrocnemius tendon
Investigations
Along with subjective and objective findings, imaging is advised prior to further treatment planning(1,3). Standard anteroposterior X-ray would show a linear soft tissue opacity medial to the femoral condyle. The linear fashion is often suggestive of calcification, but computed tomography (CT) would confirm heterotopic ossification of the femoral attachment of the MCL (see figure 4 below). Magnetic resonance imaging (MRI) helps to reveal a corticated structure within the proximal MCL, with no evidence of fat content. MRI is invaluable in defining the anatomy of the structures and confirmation of the site of calcification(1,3,5,7).Figure 4: CT scan showing heterotopic ossification of the MCL (arrowed)*
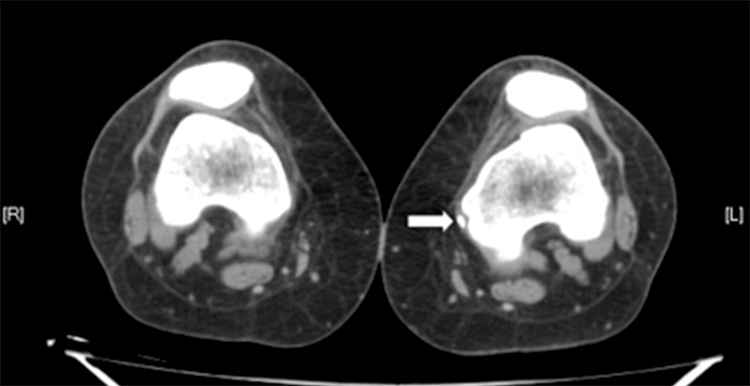
*Int J Radiology (2009); 12(2) - used with permission.
PSS treatment
Conservative treatment options should always be considered first(3). Only in severe cases should surgical intervention be offered. In this case, open surgical removal is preferred over image-guided aspiration to ensure total removal, whilst giving an accurate account of the stability of the MCL structure(1,3). Conservative treatment options include non-steroidal anti-inflammatory drugs (NSAIDs) and analgesics(1,3). If required, local corticosteroid or anaesthetic injection can be effective(1,2,3,5). Other recommendations include extracorporeal shockwave therapy(1,2)or local dry needling(1). Research supports the role of rehabilitation (together with any pain-relief medication) as a means of accelerating soft tissue healing(8), and taking advantage of the already proficient healing capacity of the MCL complex(9).Rehabilitation
Optimising the range of motion in the knee should be the first priority. This promotes joint mobility by preventing arthrofibrosis, but also by avoiding negative effects on muscular strength development, and promoting mechanotransduction(4,8).Periodised strengthening programs elicit greater strength gains than non-periodised programs, with the goal of optimising the neuromuscular systems to adapt to unaccustomed load or stressors(10). With this kind of programme, the focus should be on lower extremity as well as proximal strength, and trunk strength to promote appropriate joint reaction forces at the knee(4). Further emphasis should also be placed on hip abduction control during dynamic activities, as weakness here has been shown to place increased valgus stress across the knee(11). The following four exercises give a good grounding with the above in mind before developing sports specific rehabilitation:
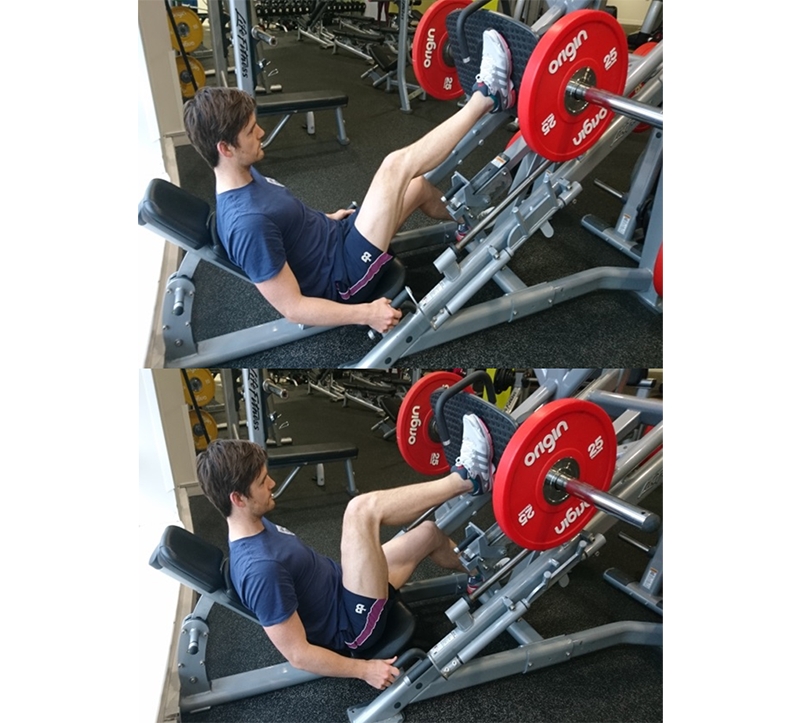
- Single-leg press: Keeping the affected knee in line with the knee. Push the resistance away from you. Return to the start position. Choose a weight where you can manage 6 repetitions (3 sets).
- Medial hamstring-biased Nordics(12):In kneeling,fix both ankles.Lean forward keeping your trunk and hips stiff and bending from the knees only. Return to the start position.Repeat 6 repetitions x 3 sets.

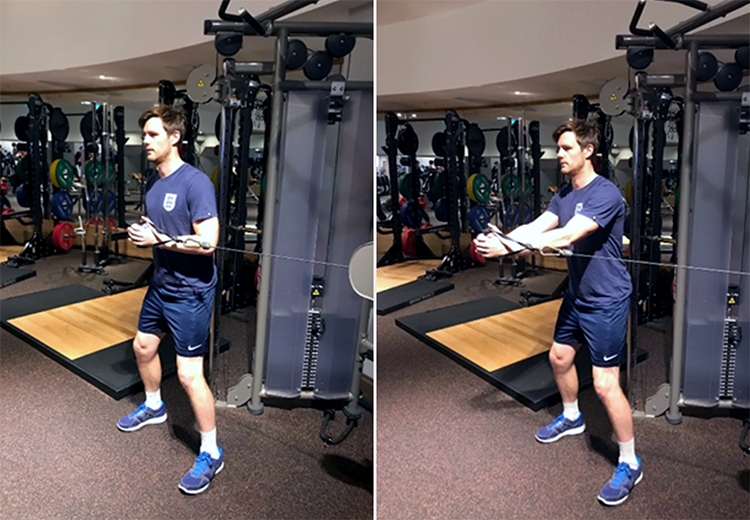
- Cable pallof press: Great for trunk rotational control, which transfers to the knee.Select an appropriate weight. The cable should be in line with the chest. Position into a shallow squat. Maintain this position and push hands away from chest. Repeat for 12 repetitions and change sides. Perform 3 sets.
- Single-leg squat off box: Great for functional hip abduction control.Sit back into a shallow squat, keeping the majority of your weight into the heel. Avoid a contralateral pelvic drop, and keep knee in line with 2nd-3rd toes. This will avoid a valgus loading mechanism. Repeat 12 reps for 3 sets.

Return to sport
Rehabilitation should include sports-specific exercise. A battery of discharge and return-to-sport tests should be used for objective assessment (see table 2). Failure of these tests were associated with a four times greater risk of re-rupture in ACL reconstructions(13). Isokinetic testing requires specific equipment in the clinic. However, all the other assessments just need space, and are a very useful objective measurement for judging an athlete’s suitability for returning to sport.| Return to sport test | Criteria for discharge |
|---|---|
| Single hop | Limb symmetry over 90% |
| Tripple hop | Limb symmetry over 90% |
| Triple crossover hop | Limb symmetry over 90% |
| Isokinetic test at 60, 180, and 360 degrees per second | Quadriceps deficit less than 10% at 60 degrees per second |
| Running t test | Under 11 seconds |
| On-field sports-specific rehab | Fully completed |
References
- Siddiq, M. A. B. & Jahan, I. (2016). Acta Radiologica Open; 6(11): 1-5
- Gelber, P. E. & Perelli, S. (2018). Ann Joint; 6(78): 1-11
- Olivier, A.C. et al (2015). Euro Jour Sp Med; 3(1): 45-51
- Logan, C.A. et al (2016). Int J Sports Phy Th; 11(7): 1177-1190
- Wijdicks, C.A. et al (2010). J Bone Joint Surg Am; 92: 1266-80
- Kamawal, Y. et al (2016). BMC Musculoskeletal Disord; 17: 283
- Wiegerinck, J.L. & Somford, M.P. (2016). JISAKOS; 1: 214-218
- Kahn, K. M. & Scott, A. (2009). Br J Sports Med; 43: 247-251
- Zhang, J, et al (2011). BMC Med; 9(1): 68
- Lorenz, D.S et al (2010). Sports Health; 2(6): 509-518
- Powers, C.M. (2010). J Orthop Sports Phys Ther; 40(2): 42-51
- Bourne, M.N. et al (2017). Br J Sports Med; 51(13): 1021-1028
- Kyritis, P. et al (2016). Br J Sports Med; 50: 946-951
Patrick Gillham

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.