You are viewing 1 of your 1 free articles
The Great Cover Up: does hopping for distance mask lower limb asymmetry?
The Great Cover Up: does hopping for distance mask lower limb asymmetry?
Single leg hops for distance have become a hallmark of return to sport decision-making following knee injuries. However, the test results can be misleading and cover up asymmetries that may impact performance or injury risk. Marianke van der Merwe discusses using single leg hop tests in RTS decision-making and provides practitioners with guidance to improve the validity of clinical testing.

Only one-third of athletes return to full competition one year after an anterior cruciate ligament reconstruction (ACLR) surgery(1). Furthermore, a reinjury rate of 24% exists among active young individuals who returned to sport within two years after an ACLR(2). In an attempt to improve return to performance outcomes, practitioners typically assess functional performance objectively and subjectively. In addition, practitioners can use some of the single leg hop tests during the rehabilitation process to provide insight into the athlete’s progress and readiness to return to training and then sport(3). These tests should measure the intended construct, detect changes over time, and be free from measurement error(3). Currently, the evidence pool lacks high-quality evidence for the measurement properties of functional performance tests for athletes recovering from ACLR(3).
Functional performance tests objectively quantify lower limb function while assessing progress within the rehabilitation process(1). Quantity of movement refers to force production capabilities, whereas quality refers to the range in which the limb moves(4). These tests are easy to administer, require minimal equipment, are not time-consuming, and can be performed almost anywhere(5). The selected tests must be reliable, valid, standardized, and sensitive to detect small changes(4,6). There is a range of different functional performance tests that practitioners can use to assess an athlete’s readiness (see table 1). However, the reliability and validity of these tests are variable and may misrepresent an athlete’s capabilities.
Table 1: Brief description of included functional performance tests(3).
|
Functional performance test |
Activity |
Quantification measure |
|
Single Leg Hop |
Horizontal hop |
Length (cm) |
|
6m Timed Hop |
Hop for 6m |
Time (sec) |
|
Crossover Hop |
Three crossover hops |
Length (cm) |
|
Triple Hop |
Three hops |
Length (cm) |
|
Vertical Hop |
Vertical hop |
Height (cm) |
|
Single Leg Drop Jump |
Drop, vertical hop |
Height (cm) |
|
4-Jump Vertical Hop |
Four vertical hops |
Height (cm) |
|
Vertical Jump |
Vertical jump |
Height (cm) |
|
Medial Hop |
Sideways hop in a medial direction |
Length (cm) |
|
Lateral Hop |
Sideways hop in a lateral direction |
Length (cm) |
|
Timed Speedy Hop |
Forwards, backward, and sideways hops (Agility course) |
Time (sec) |
|
10s Vertical Hop |
Vertical hops for 10s |
Height (cm) |
|
Stair Hop |
Hop up then down three steps |
Time (sec) |
|
Step-Down |
Step down on one leg (60s) |
No. of reps. |
|
Carioca |
Lateral crossover steps |
Time (sec) |
|
Shuttle Run |
Run back and forth |
Time (sec) |
|
Side-Step |
Run laterally |
Time (sec) |
|
Co-Contraction |
Run with a Velcro belt |
Time (sec) |
|
Star Excursion Balance Test |
Dynamic single-leg balance |
Length (cm) |
|
Y-Balance Test |
Dynamic single-leg balance |
Length (cm) |
|
Test Battery Vertical Hop Single Leg Hop Drop Jump Square Hop Side Hop |
Vertical hop Horizontal hop Drop and then two horizontal hops Hop in and out of a square (30s) Lateral hops over 40cm (30s) |
Height (cm) Length (cm) Length (cm) No. of reps. No. of reps. |
Functional performance testing
The Single Leg Hop is the most commonly used functional performance test, which displays good intrarater reliability(3). Furthermore, sufficient (moderate) intrarater reliability exists for 6m Timed Hop, Crossover Hop test, and the Vertical Hop test. On the contrary, for the Triple Leg Hop and Stair Hop, the quality of evidence is very poor, and conclusions are difficult to draw(3). Notably, practitioners need to be cautious when comparing results of the 6m Timed Hop as inter-rater reliability when using the Limb Symmetry Index (LSI) as an outcome may be poor. In the clinical setting, the low reliability may challenge practitioners to gain meaningful insight into an athlete’s capabilities. However, there are strategies to improve reliability and give practitioners greater confidence in the test results. These strategies include practitioner training in the measurement procedures, athlete familiarization through repeated exposure throughout the rehabilitation process, and averaging the measures (e.g., averaging three hops per side)(3).
Another method to enhance the meaningfulness of the test results is the Limb Symmetry Index. The LSI provides a measure of the performance of the involved limb with the uninvolved limb. The LSI values may also be more consistent than absolute values as it accounts for the learning effect(3). However, practitioners must be cautious when interpreting the results using LSI, as generalized deconditioning following injury may result in deficits in the uninvolved limb, particularly when comparing the results to population norms.
The hop tests demonstrate moderate to strong associations with quadriceps strength(3). However, the validity and relation to knee muscle strength following injury is questionable due to the possibility that athletes can utilize compensation strategies to maximize their outcomes. For example, following ACLR, the knee only contributes 12% to the propulsive phase of the Single Leg Hop test, and knee biomechanical asymmetries exist despite between-limb hop distance symmetry(7). Therefore, practitioners should consider the hop tests as measures of total lower extremity function instead of only the knee joint or single muscles.
The modified Star Excursion Balance Test (SEBT) is reliable, valid, and sensitive to detect dynamic postural control deficits and indicates muscle strength, power, neuromuscular control, and confidence in the ACL-deficient (ACL-D) limb(6). Patients with ACL deficiency portray functional deficits in the anterior, medial, lateral, and posteromedial reach directions(6).
___________________________________________________________________________
Reliability vs. Validity
Reliability and validity are both about how well a method measures something. Reliability refers to whether the test results can be reproduced under the same conditions (consistency). Validity refers to whether the results represent what they are supposed to measure (accuracy).
___________________________________________________________________________
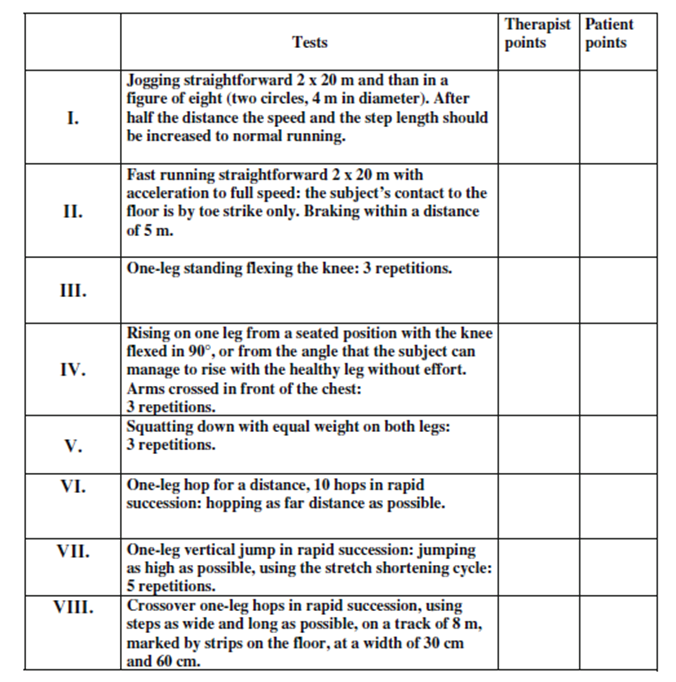
The test of athletes with knee injuries (TAK) is a criterion-based test used to evaluate the patient’s quality of functional knee performance during rehabilitation(6). Consisting of eight different functional activities emphasizing stability, strength, springiness, and endurance(6). The physiotherapist visually observes and rates (criterion-based scale of 0-5) the tests performed while the patient simultaneously rates their performance experience of the tests (scale of 0-10) (see figure 1)(6). The TAK test has good inter-rater and acceptable intra-rater reliability(6).
Figure 1: TAK assessment form(6)
Related Files
Isometric quadriceps femoris (QF) strength is measured using a maximal voluntary isometric muscle contraction (MVIC) on an electromechanical dynamometer(1,2). The quadriceps strength is reported as quadriceps index (force of involved limb/ force of uninvolved limb x 100)(6). Quadriceps femoris strength deficits greater than 15% on the involved limb negatively affect function and performance(6). This emphasizes the importance of quadriceps strength and how it influences knee function.
Subjective functional performance tests
The athlete’s voice is essential to the return to sport (RTS) readiness evaluation. Practitioners can gather subjective information via questionnaires that athletes complete as part of the RTS assessment. In addition, athletes should provide information regarding their functional ability and perception of the symptoms that they experience(1,6). The International Knee Documentation Committee subjective knee form (IKDC), Knee Injury and Osteoarthritis Outcome Score (KOOS), and Knee Outcome Survey-Activities of Daily Living Scale (KOS-ADLS) are used extensively in the literature. Combining subjective and objective information aids in the process of developing personalized rehabilitation plans.
Meaningful data
Practitioners need to identify when differences, either between limbs or in comparison to population norms, are meaningful. They can interpret the valuable data gathered through testing utilizing the minimal important change (MIC) and LSI. The MIC is the smallest meaningful change detected in a score(5). The LSI is a calculation used to indicate the percentage difference between the injured and non-injured limb, and scores need to be more than 90% to be considered normal(3,4). For example, with the Single Leg Hop test, the minimal important change is 6.7% and 9.7%(8,9). This indicates that differences in LSI scores above 10% represent a real difference. The other hop tests have slightly higher values, i.e., 6 m Timed Hop (15.5%), Crossover Hop (14.6%), and Triple Hop (12.0%) tests(3).
Return to sport complexity
Return to sport readiness is a complex interplay of physical and biopsychosocial factors. Therefore, practitioners should combine the objective and subjective assessments to create a holistic decision-making tool and continuously evaluate athletes throughout rehabilitation to better understand their needs and prognosis. In 2018, researchers at the University of Delaware, in the USA, aimed to investigate whether return to activity criteria, individually or in combination, at six months after ACLR can predict a RTS at preinjury activity level at 12 and 24 months.
The researchers assessed the isometric quadriceps index, LSI using multiple single-legged hop tests, and the KOS-ADLS questionnaire to establish a specific return to activity criteria. The researchers defined the PASS group as scoring >90% on all criteria and the FAIL group as scoring <90% on any criteria. The researchers then contacted the participants at 12 and 24 months after ACLR to ask if they returned to sports at the same preinjury activity level.
At six months post ACLR, individuals who portrayed normal limb-to-limb movement and knee function during functional tasks were more likely to return to preinjury activity at 12 and 24 months(1). Single-legged hop tests were consistent predictors of outcome at both 12 and 24 months, while patient-reported measures only predicted the outcomes at 12 months(1). The researchers found that the RTS rates at the same preinjury activity level at 12 and 24 months after ACLR were higher among participants who passed the return to activity criteria than those who failed six months after ACLR(1).
Furthermore, the researchers used the 6m Timed Hop test as a decision-making tool to determine which individuals can return to high-level activity without surgery after an ACL rupture(1). The 6m Timed Hop test was the strongest predictor at 12 and 24 months(1). Therefore, it might be easier for participants to perform a series of consecutive hops over a 6 m distance as fast as possible without changing the direction, controlling their landing, or stopping their body momentum, as is the case in hop tests for distance.
Conclusion
Using multiple hop tests increases the ability to detect discrepancies in performance and reflects the integrated effect of strength, neuromuscular control, and limb confidence with minimal equipment and time needed(1,4). In addition, return to activity criteria aid in RTS decision-making and help to identify any functional and limb-to-limb deficits(1,4). Practitioners can tailor the rehabilitation program using these objective measures to include the necessary strength, power, and neuromuscular exercises to regain optimal function and performance.
Although there is a lack of high-quality evidence to support the reliability and validity of various lower limb performance tests, practitioners still have to make decisions with the tools at their disposal. Continuous and reproducible assessments are key to evaluating RTS readiness. As athletes progress through the RTS continuum, practitioners should continuously assess their subjective and physical readiness with multiple tests to assist the return to performance decision-making puzzle.
References
- Br J Sports Med 2018;52:375
- J Orthop Sports Phys Ther. 2012 Sep;42(9):750-9.
- Br J Sports Med 2022;0:1-12
- ISRN 2014, Article ID 613034, 14 pages
- Br J Sports Med 2015;49:642-648
- Knee Surg Traumatol Arthosc 2009; 17:435-445
- Br J Sports Med 2022;56:249–56.
- Phys Ther 2007;87:337–49
- Knee Surg Sports Traumatol Arthrosc 2002;10:10–19

Marianke van der Merwe

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.