You are viewing 1 of your 1 free articles
Neuroplasticity in sports injury rehabilitation: Part I
In the first part of a 2-part article, Chris Mallac explores the concept of neuroplasticity, and how a better understanding of its underlying principles improves rehab outcomes.
Reinjury rates following return to sport are often quite high. In under-25 athletes for example, the incidence of another anterior cruciate ligament (ACL) rupture (or ACL failure) run as high as 23%(1). The reasons for reinjury when returning to sport are multifactorial. One of the commonly identified factors is a failure to target and retrain motor control resulting in aberrant movement patterns in the recovering athlete. Despite attempts at best practice rehabilitation of athletes, the utilization of motor control principles - specifically the principles of neuroplasticity - is frequently neglected.
What is neuroplasticity?
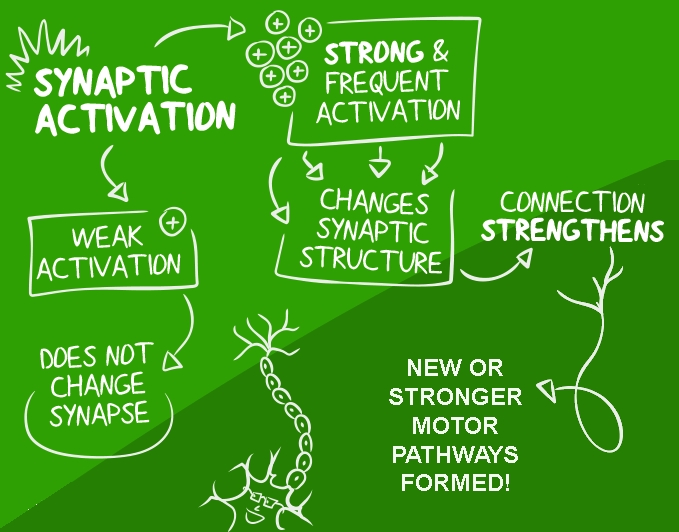
The Polish neuroscientist Jerzy Konorski most likely coined the term neuroplasticity. In 1948, he described the adaptive cellular mechanisms of learning. He observed that learning occurred through a change in the quality of the connections between neurons in the brain. Those connections which were strengthened through frequent activation allowed encoded memories (see figure 1)(2). Many additions and revisions of this concept transpired over the next few decades. Ultimately rehabilitation professionals harnessed the concept of plasticity, or the ability of the brain to change the wiring of neural networks, in the recovery of central nervous system disorders. Indeed, many of the current modern-day rehabilitation programs used for traumatic brain injury and cerebral vascular accidents (strokes and aneurysms) have their roots embedded in the original theories proposed by Konorski.

Figure 1: A simplified concept of motor neuroplasticity in terms of synaptic activation
The application of the concept of neuroplasticity extends beyond the realm of purely neurological therapy. This model has a place in the rehabilitation of sports injuries as well. For instance, ACL tears, shoulder instability, broken long bones, or ankle fractures are time-dependent injuries. Part of the extensive rehabilitation of these injuries is the recovery of motor control, which is governed by the central nervous system.
Jeffrey Kleim and Theresa Jones presented a detailed synopsis on the use of the exercise dependent principles of neuroplasticity in 2008(3). The 10 key principles outlined, and discussed here in the context of sports injuries, are as follows:
- Use it or lose it
- Use it and improve it
- Specificity
- Repetition matters
- Intensity matters
- Time matters
- Salience matters
- Age matters
- Transference
- Interference
- Use it or lose it
Research on those who lose a sensory function shows that unused neural circuits are reassigned to another part of the sensory or motor cortex. When a person loses their vision, the brain reassigns the neurons used for vision to tactile sensations. This redistribution of neurons explains why blind persons become so skilled at Braille reading(4). Rehab professionals sought ways to prevent this reassignment of neurons when a limb temporarily loses its ability to function after an injury.
Those who work in the field of stroke rehabilitation medicine discovered that by restraining the affected limb and using the unaffected limb to perform rehabilitation activities, the affected limb improved in function. Strangely, this mirrored activity in the functioning limb activates the remaining neurons of the stroke affected cortex(5). This phenomenon is called cross-education(6).
Physiotherapists can utilize this concept in the rehabilitation of ACL tears. Immediately following the injury, begin resistance activities on the uninjured limb. The injured leg makes strength gains despite not participating in the exercise program.
- Use it to improve it
The assignment of the appropriate rehabilitation activities with adequate dosing depends on an understanding of the neural mechanisms involved. For example, athletes with chronic ankle instability (CAI) have a delayed contraction reaction in the peroneal muscles when they experience an inversion perturbation. The delay in impulse transmission at the neuromuscular junction of the peroneal muscles, or latency, is about 26% longer than uninjured ankles(7).
This latency is likely due to an alteration of joint mechanoreceptor activation. Theoretically, the mechanoreceptors trigger short reflex pathways and muscle spindle activation. This altered reflex activity changes the gamma motor neuron feedback loop and thus the neuromuscular firing(7). This pathway acts over the short spinal level reflexes and does not involve the higher brain centers.
However, balance and position sense are mediated through the cerebral cortex and cerebellum by the integration of visual and vestibular sensory input through complex neural networks in the cerebral motor cortex. Joint mechanoreceptors, needed to trigger the spinal reflex activity, receive efferent input from the central nervous system that can make them more sensitive and responsive. Therefore, balance and position sense training is needed to increase the cerebral involvement to negate this delay in the spinal reflex loop.
Through a process known as synaptogenesis, the cerebral cortex increases synaptic responses within a cortical area due to repetitive skill training (see figure 1)(3). The neural plasticity concept of ‘use it to improve it,’ means that injured athletes must continue to train a modality such as balance and reactivity - even after they have returned to play - to recover the capacities of balance and proprioception further. This training may exceed the dosages of practice recommended for uninjured athletes
- Specificity
Clinicians often ignore this seemingly obvious principle when prescribing rehabilitation exercises. Many rehabilitation programs are ‘copy and paste’ type programs that are not bespoke enough for an individual athlete, in a specific sport, with a particular injury. Merely performing a random movement (motor use) is not as effective in creating cortical changes as actually performing a skill (motor learning).
A simple example is regaining quadriceps strength after ACL reconstruction. Performing isolated quadriceps loading exercises such as leg extensions and single-leg squats may be adequate for restoring quadriceps mass following surgery; however, this does not translate to the functional use of the quadriceps in controlling deceleration forces during sport. To obtain this control, the athlete needs to perform specific deceleration and landing drills.
A graduated deceleration program starts with simple landings from a height and progresses to performing the sport-specific landing tasks. Compare a volleyball player who needs to land from a vertical jump after a spike or a block at the net, with a running back in the national football league (NFL), who often needs to stop and change direction quickly in a horizontal direction. Both tasks need deceleration but in different planes of movement. A basketballer using the rehabilitation program of a famous NFL running back will not develop the same level of cortical reorganization following injury because the rehabilitation exercise of choice is not specific enough for their needs.
- Repetition matters
This principle fits with the adage that recommends 10,000 hours of practice needed to develop a skill. Injured athletes may need to increase an aspect of training or rehabilitation over and beyond the usual dosage to sustain a beneficial response. Repetition of a newly learned or relearned task is required to gain long lasting neural changes in the cerebral cortex(3). Through repetition, skills become more enduring and accessible within the neural networks of the cerebral cortex(8).
Repetition promotes neural reorganization and the ability to access and use the newly acquired skill or functional motor pattern even after the completion of rehabilitation. Professional athletes typically have enough supportive resources to help them with supervised and regular repetition. However, recreational athletes who only attend physiotherapy once a week or fortnight need guidance on the correct dosage and frequency of exercises to perform outside of formal rehabilitation.
- Intensity matters
Along with repetition, the intensity of the training used in recovery training also influences the speed at which permanent neural networks are formed and retained. Intensity can be modulated either through load (using heavier weights), speed (moving faster), or density (performing more reps in a defined period). All three methods challenge the neural drive and thus lead more rapidly to longer-lasting changes in neural connectivity.
Consider an example of a surgically stabilized Lisfranc’s injury. Once the athlete removes the motion control boot, they will have lost a great deal of strength and size in the calf muscle complex. Rehabilitation therapists prescribe calf-raise exercises to regain muscle size and strength. The typical protocol recommends bodyweight calf raises for three sets of 15 repetitions, often with an eccentric focus such as a counting one up and two down format. These exercises alone lack the intensity to build the neural connections needed for rapid force production. Therefore, modulating the variables of intensity such as load by performing loaded calf eccentrics, speed using plyometrics jumps and landings, and density with shorter rests between sets, help regain this capacity.
In summary
Athletes who aim to return to their previous level of function following a long-term injury do not always regain total pre-injury function. The consequence is the inability to return to their pre-injury level of competition or reinjury. Rehabilitation programs often fail to equip athletes with a robust injury-resistant body because they do not adequately address the concepts of neuroplasticity and motor relearning. Athletes do not need cookie-cutter protocols; rather, they require bespoke programs that adequately suit their functional needs and utilize the concepts of neuroplasticity.
In part two of this article, we will explore the five remaining exercise-dependent principles of neuroplasticity, and how they impact sports rehabilitation.
References
- Am J of Sports Medicine. 2016. 44(7); 1861-1876.
- Eur J Neurosci. 2019; 00:1–10.
- Journal of Speech, Language and Hearing Research. 2008, 51. S225-s239
- 1996. 380, pp 526-528.
- Physical Medicine and Rehabilitation Clinics of North America. 2003. 14(supp 1), S77-91.
- Sports Medicine. 2007. 37 (1): 1–14
- Journal of Orthopaedic Research. 2009. 27(12); 1541-1546.
- Neuroscientist 2005. 11. 471-483.

Chris Mallac

Latest Issue

Subscribe Today
Further reading
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.