You are viewing 1 of your 1 free articles
Mind the gap: Diastasis recti in postpartum athletes

Female athletes often experience the peak of their physical performance and their optimal fertile age simultaneously. Many female athletes continue to train during pregnancy and the postpartum period - but even elite female athletes are not exempt from the typical musculoskeletal issues that can arise during pregnancy. These issues may be aggravated in athletes who experience vigorous loading and high volumes of impact or exertion. In these circumstances, elite female athletes can experience persistent postpartum diastasis recti (DR).
Diastasis recti refers to the separation of the outermost abdominal muscles due to the thinning and widening of the line alba (the connective tissue between the two muscle bellies of rectus abdominus)(1). The criteria for the diagnosis of DR is a separation or gap of more than 1.5cm at one or more points of the linea alba, (see figure 1)(2).
Figure 1: Linea alba and observed patterns of diastasis recti*
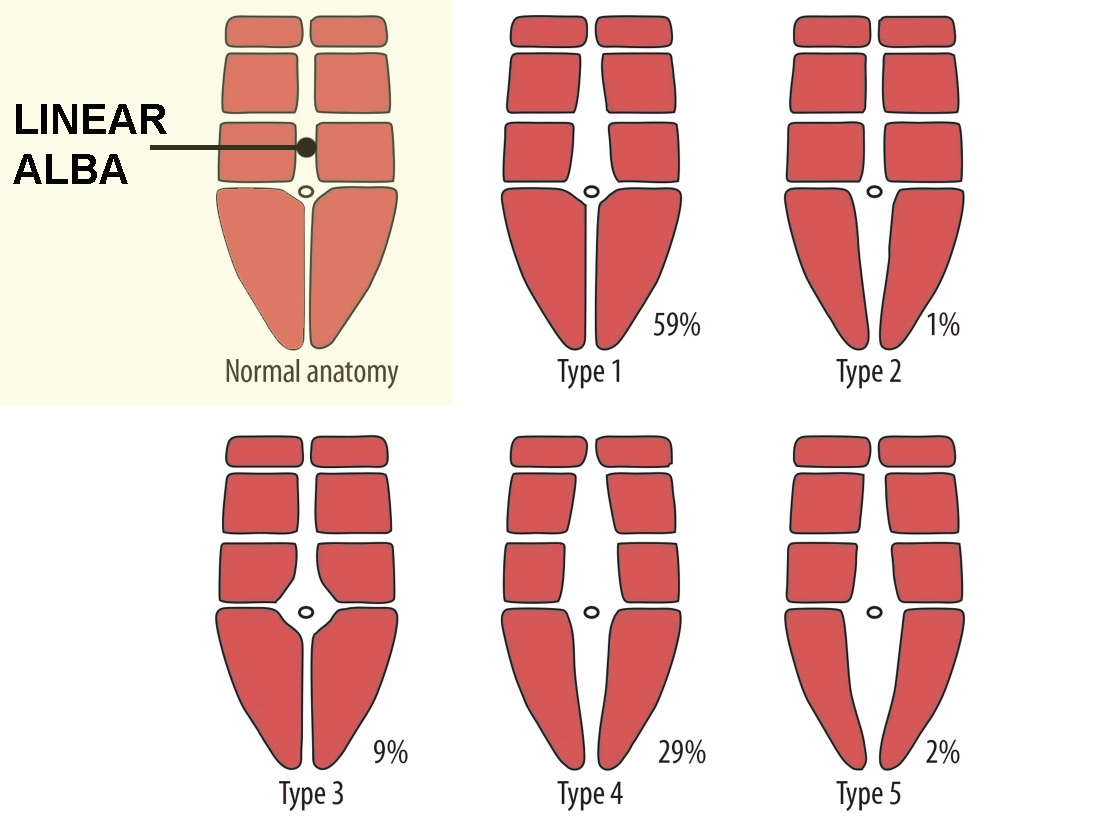
The ‘normal’ panel (top left) shows the typical anatomy with the linea alba. Patterns of separation can vary. In a study of 92 women by Corvino et al 2019, researchers identified five distinct patterns: pattern 1 - only above navel (58.5%); pattern 2 - only below navel (1.2%); pattern 3 - at navel level (8.5%); pattern 4 - complete but wider above navel (29.3%); pattern 5 - complete but wider below navel (2.4%).
*diagram adapted from Corvino at al [Pol J Radiol. 2019; 84: e542–e548].
Diastasis recti can occur as early as week 14 in pregnancy, and by week 35 of gestation, 100% of women will experience some DR(3,4). Approximately half of these resolve spontaneously postpartum, or within the first eight weeks(5). However, up to 45% of women may have DR that remains at six months postpartum and 32% at 12 months postpartum(6). When DR fails to resolve in a timely fashion, some conservative management interventions can help.
Anatomy and function
The abdominal muscles support the internal organs, and the linea alba (see figure 1) maintains the mechanical stability of the abdominal wall. It is the central tissue that connects the fascia covering the rectus abdominis muscle and is the insertion point for all three abdominal muscles(7). Collectively, the fascia and muscles help support the pelvis and lumbar spine.As the pregnancy develops, the growth of the uterus and accompanying hormonal changes cause an alteration in the elasticity of the connective tissue, which results in a displacement of the abdominal wall(7,8). As the uterus expands outwards, the pelvis compensates by tilting anteriorly, which elongates the abdominal and pelvic floor muscles and stretches the linea alba(7). This change in posture reduces the integrity, mechanical control, and strength of the abdominal muscles.
The abdominal muscles, including the deep transversus abdominis (TVA), the pelvic floor muscles, the multifidus, and the diaphragm work together to provide stability to the trunk; therefore, dysfunction in one of these influences the function(s) of the other(9). During physical exertion, increased intra-abdominal pressure (IAP) can cause the anterior abdominal wall to bulge at the location of the DR(8). This weakness can affect the transfer of load through the lumbar spine and pelvis, leading to low back and pelvic pain.
Diastasis recti is also linked to pelvic floor muscle weakness. Pelvic floor weakness can lead to incontinence and pelvic organ prolapse. A study conducted at Andrews University found that in those with urological disorders, approximately half had DR, and 66% had pelvic floor dysfunction(10). Because DR is associated with pelvic floor instability and incontinence, treatment should include an investigation of the entire abdominal girdle. A patient may come into the clinic because they don’t like the ‘pooching’ in their stomach, but not mention the other pelvic floor issues out of embarrassment. Therefore, every complaint of DR, even in the early postnatal period, warrants a full evaluation and treatment plan.
Assessment of a diastasis recti
Previous DR assessments have focused solely on measuring the gap between the rectus abdominis muscle bellies. However, this does not provide information on the tensile strength and function of the abdominal wall, or the individual’s ability to control the muscles. This knowledge is fundamental to returning an athlete to function. Therefore, a more astute evaluation should include:- Tension - Tension occurs when the core and pelvic floor are engaged, and the region becomes taught as the muscle contraction takes up slack. Ideally, measure the tension in standing. Initially, palpate the line alba without any contraction to identify firmness, width of gap, and depth.
- Determine measurements - Quantify your assessment on a scale of one to five, with one being very poor and five being excellent in terms of muscle quality, firmness, and depth of softness.
- Repeat with engagement - Repeat step one, but this time engage the core and pelvic floor while palpating the line alba. Identify any changes in comparison.
- Compare in different positions - Repeat the process in different positions to identify if the athlete can control their abdominal tension throughout, or if they lack strength in a specific postures.
PPP-RL-LD
Follow the initial examination of the muscle integrity with an assessment of other factors indicated by the acronym PPP-RR-LD(11). This stands for:- Person: Establish the individual’s history with diastasis, goals, and rehabilitation expectations to personalize their treatment plan.
- Posture: Body position affects DR and influences the intra-recti distance (being wider in upright positions)(12). Some postures may also affect muscle recruitment so evaluate DR’s severity in a range of different postures.
- Patterns: Compensatory patterns, such as rib flaring, abdominal gripping, or overactivity of the oblique muscles, may develop due to the reduced abdominal muscle function. All of these may impact the pelvic floor and reduce the efficiency of normal movement.
- Respiration: The diaphragm’s involvement in the synergy of core control is important to restore coordination and management of IAP. Exhalation also improves recruitment of the TVA, thus use breathing patterns as a strategy to influence muscle activity(13)
- Ribcage: The ribcage expands outwards during inhalation and provides dynamic assistance during muscle activity. However, rib flaring during a loaded exercise is a compensation strategy and highlights abdominal weakness.
- Load: Progressive loading stimulates adaptation in the muscles of the abdominal wall. Begin with the maximum loading the athlete can withstand without compensation, ie. with no doming or deviation from a neutral lumbopelvic position (see figure 2).
- Defect: The DR may exacerbate postpartum defects in the abdominal wall, such as hernias. Refer these patients to a physician for diagnosis and treatment before proceeding with DR rehabilitation activities.
Treatment
Simply activating core muscles isn’t enough to resolve DR. While rectus abdominis activation via an abdominal curl-up reduces the intra-abdominal distance of the DR, it also distorts the linea alba. This distortion produces less tension and an inefficient transfer of loads across the pelvis. Contraction of the TVA widens the gap; however, if the TVA is pre-activated before the rectus abdominis, the combined effect is a closure of the gap and prevention of linea alba distortion.Therefore, focus the initial treatment on the recruitment of the deep core muscles. Then, progressively load the abdominals to induce muscle hypertrophy and increase metabolic demand. The results of a progressive strengthening program include increased strength, endurance, and power capacity. A program of eight weeks of deep-core stability exercises produces significant reductions in the intra-rectus distance (the anterior muscle gap) and improves the quality of life(7).
That said, a return to full strength and integrity can take much longer than the average muscle hypertrophy timeframe of 12 weeks. The linea alba lacks an abundance of collagen fibers. Thus, adaptation and remodeling of the connective tissue can take up to two years(14).
Figure 2: Abdominal doming
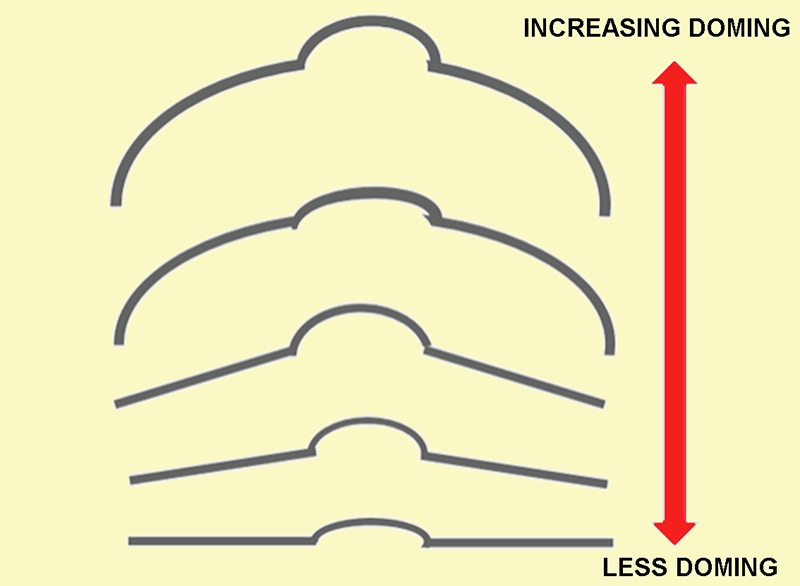
Doming occurs when there is an increase in IAP, and the abdominal wall cannot manage the pressure sufficiently. This outpouching of the abdominal wall occurs on a continuum (see figure 2). Rather than preventing an athlete from completing an exercise if doming occurs, adapt the exercise instead. Modifying the level and technique of core engagement, breathing pattern, and posture can reduce doming and provide increased abdominal control. Progress exercises gradually to ensure correct activation and control before advancing to the next harder level.
Rehabilitation exercises for diastasis recti
Primary activation: Start with foundational exercises to ensure coordination, activation, postural awareness, and the ability to control the load with the abdominal wall.- Core and pelvic floor activation (see figure 3): Begin in crook lying. Engage core approximately 30% and lift pelvic floor from the back passage, middle, to front passage, then fully release. A soft ball between the knees helps with awareness of these muscles.
- Double-leg stretch (see figure 4): Extend both arms overhead and simultaneously extend one leg away from you. Use the core to return, maintaining a neutral trunk.
- Abdominal preparation (see figure 5): Lift upwards from the core, keeping a neutral spine until the shoulder blades are almost off the floor. Return to starting position.
Figure 3: Core and pelvic floor activation

Figure 4: Double-leg stretch

Figure 4: Abdominal preparation

Functional activation: A DR causes trunk rotation and flexion deficits; therefore, rehabilitation should address these by loading in these specific movements. These are also functional for everyday life and essential to every sporting activity. This video explains the functional movements and exercises to restore them. Subscribers, find the video here:
[leaky_paywall_not_subscriber]
 [/leaky_paywall_not_subscriber]
[/leaky_paywall_not_subscriber][embed]
[leaky_paywall_subscriber]
In summary
Diastasis recti is a separation of the anterior abdominal muscles and thinning of the linea alba, and occurs in 100% of women by the third trimester. Around half of the cases resolve naturally, while the rest require rehabilitation. Prioritize DR rehabilitation within the first three months postpartum to avoid adverse changes in posture, pelvic floor dysfunction, and low back pain. The assessments should measure tension at rest and upon abdominal activation, and then expanded using the acronym PPP-RR-LD. Treatment should maximize the pre-activation of the TVA before the rectus abdominis contraction. Make the abdominal strengthening program functional and prescribe the maximum load achievable with control of doming and lumbopelvic stability.References
- J of Pelvic, Obst and Gynaecol Physiother. 2019; 124:15-19.
- Clinical anatomy, 2009. (6):706-711.
- Phys Ther, 1996;76:750–62.
- Manual Therapy, 2015. (1):200-205.
- Manual Therapy, 2008. 13(2):112-121.
- Br J Sports Med. 2016;50:1092-1096.
- J Musculoskeletal Neuronal Interact. 2019; 19(1):62-68.
- Ginekologia Polska. 2018; 89(2):97-101.
- J Phys Therapy Science. 2015; 27(7): 2113-2115.
- J Womens Health Phys Therap. 2009;33(2): 15-22.
- J Pelvic, Obst and Gynaecol Physiother. 2019; 124: 15-19.
- Musculoskel Science and Practise. 2018; 34:1-7. DOI: 10.1016/j.msksp.2017.11.010
- Neurourology and Urodynamics. 2007; 26(3): 362-371.
- Clinics (Sao Paulo). 2018; 73: e319.

Tracy Ward

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.