You are viewing 1 of your 1 free articles
The Lesser Known Morel-Lavallée Lesion
Morel-Lavallée lesions are closed degloving soft tissue injuries characterized by the separation of the skin and underlying tissue layers due to shearing forces. Candice MacMillan summarizes the pathophysiology, clinical presentation, diagnosis, and treatment of MLLs.

South Africa’s Sisanda Mangala falls to avoid a run out REUTERS/Siphiwe Sibeko.
In sports, Morel-Lavallée lesions (MLL) are associated with low-grade blunt force trauma related to falls and contact sports, such as football and wrestling. The injury is a post-traumatic closed degloving injury where skin and superficial fascia separate from the deep fascia, creating a potential space where blood and lymph accumulate(1-4). If not treated in the acute or early sub-acute stages, fluid accumulation is at risk for superinfection, overlying tissue necrosis, and continued expansion(1,3). Early, accurate diagnosis and treatment are vital.
Causes and Pathophysiology
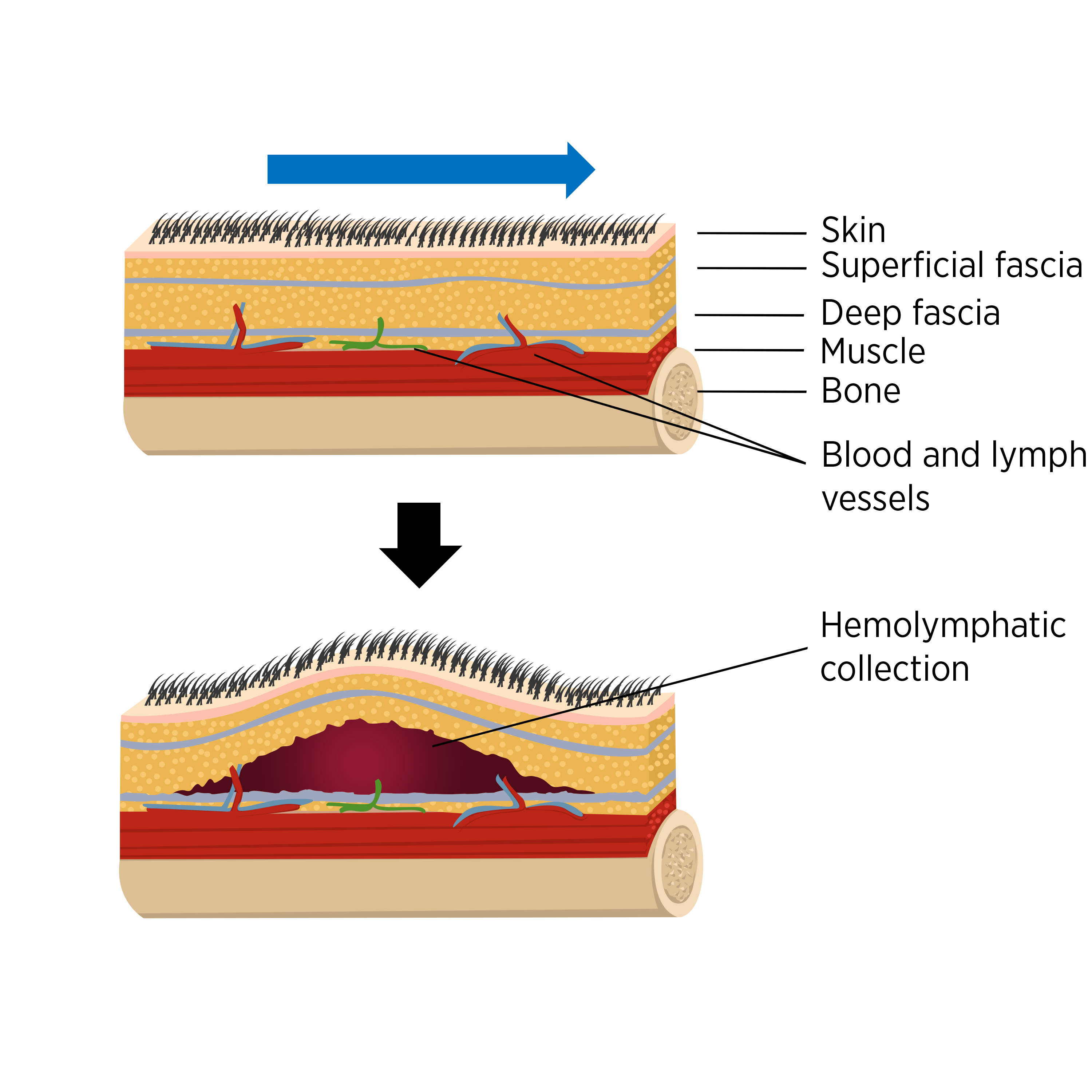
The mechanism of injury is usually trauma that occurs tangential to fascial planes, resulting in a shearing type of injury(1-3). The superficial tissues (subcutaneous fat and dermis) are more mobile than the relatively firm and immobile deep fascia and muscle, subjecting these tissues to shearing injury(1-3). Shearing forces also lead to the perforation of vascular and lymphatic structures, resulting in the accumulation of hemolymphatic fluid in the potential space generated by the separation of the superficial and deep fascia (see figure 1)(1,3).
.")
Diagnosis and clinical presentation
Diagnosis requires a comprehensive history and physical examination alongside imaging modalities, typically ultrasound or MRI. The differential diagnosis for Morel-Lavalee lesions includes sarcoma, hemorrhagic prepatellar bursitis, simple soft tissue hematomas, superficial bursitis, or necrotic soft tissue neoplasms(1-3).
History and physical examination
These injuries mainly occur due to blunt trauma after falls, motor vehicle accidents, and sport-related injuries(1,2,4-6). Post-operative cases following liposuction have also been reported(2,5). They often present soon after the inciting traumatic event, although some patients may have delayed presentation.
Clinical presentation
Lesions occur most commonly over the greater trochanter, buttock, thigh, and knee (see figure 3)(2,5,7).
The most common symptoms include(1,2,4,5,7):
- Soft, fluctuant area of contour deformity (swelling), which may have skin mobility.
- Localized tenderness due to the pressure effect of the large volume of serosanguinous fluid within a well-defined space (see figure 4).
- Bruising can take several days to develop.
- Decreased cutaneous sensation is often associated with the skin over the area of degloving because of shearing injury to the cutaneous nerves.
- Athletes may present with skin necrosis over the degloving area.
- Associated joint stiffness. However, in some cases, the affected joint has a complete and pain-free range of motion.
- Overlying soft tissue infection or skeletal fracture. The absence of prompt diagnosis and treatment may lead to secondary infection (e.g., cellulitis). The lesions can occur in isolation but are frequently associated with underlying fractures.
")
.")
Investigations
Clinicians can request ultrasound, MRI, or CT scans to diagnose MLL(1,2,4,5). On ultrasound, an elevation of the subcutaneous fat layer and superficial fascia layers from the deep fascia causes a fluid collection, which presents as an anechoic (dark) lesion on both longitudinal and transverse ultrasound imaging(1,2).
Magnetic Resonance Imaging is the modality of choice for characterizing MLLs(1,2,5). Six types of Morel-Lavallée lesions have been described based on the chronicity and composition of the collections and their MRI appearance (see table 1)(1,2,4).
Table 1: Morel-Lavallée lesion classification(1,2).
| Type | Definition |
| Type I | A serohematic effusion (seroma). |
| Type II | A subacute hematoma. |
| Type III | Is a chronic organizing hematoma. |
| Type IV | Closed fatty laceration complicated by perifascial dissection. |
| Type V | A perifascial pseudonodular lesion. |
| Type VI | An infected lesion with sinus tract formation, internal septations, and a thick enhancing capsule. |
Treatment
Clinicians should consider several factors when determining the approach to managing an MLL. The lesion size, severity, and proximity to an intended surgical incision for coexisting injury will determine the treatment selection(4). Management includes conservative treatment, minimally invasive treatment, and surgical intervention(1,3,9).
Conservative treatment
Lesions with small fluid collections and no overlying pressure changes or underlying fractures can be managed conservatively by compression bandaging and physiotherapy(1,9,10). Compression bandaging is vital as a form of primary treatment(1,3,4,9). For hip and buttock lesions, tight cycling shorts may provide adequate compression(9). Clinicians must educate patients on re-bandaging and recognizing the signs of infection to avoid complications(9).
Physiotherapy is essential for the best functional outcomes after surgery or conservative management. Rehabilitation helps in reducing pain and regaining functional activities by improving joint ROM, strength, and cardiovascular fitness (see table 2)(10).
Table 2: Post-surgical MLL debridement physiotherapy intervention(10).
| Intervention | Description | Aim |
| Patient Education. | Education regarding the condition, surgery, and prognosis. | Manage patient expectations and mental health. |
| Cardiovascular and respiratory training. | Breathing exercises. | Relaxation. Maintain cardiorespiratory well-being. |
| Bed exercises and mobility. | Practice bed mobility and progress to mobility with or without walking aids. | Regain function following surgery. |
| Joint mobility in unaffected joints. | Maintain joint mobility in unaffected joints while respecting tissue healing and surgical restrictions. | Maintain joint mobility. |
| Strengthen unaffected limbs. | Perform adequate strength training in unaffected joints. | Prevent deconditioning during recovery. |
Minimally invasive treatments
Minimally invasive treatment options include aspiration or incision and evacuation, with or without injection of sclerosing agents(1,5,9). Clinicians may use ultrasound-guided aspiration on acute lesions with fluid below 50ml(4,5,9). The MLL is aspirated to dryness and then compressed with an elastic dressing. Further aspiration may be required if fluid reaccumulates.
When aspiration fails, sclerodesis prevents fluid collection and reduces the risk of recurrence post-aspiration(5,9,11). Sclerodesis agents (oxycycline, erythromycin, bleomycin, vancomycin, absolute ethanol, tetracycline, and talc) cause cell destruction within the lesion’s periphery, which induces fibrosis(11).
Surgery: Open drainage and debridement
If initial percutaneous drainage fails, the skin overlying the lesion is necrotic, or the initial lesion is associated with an underlying open fracture, then open debridement and primary closure are indicated(5,9,11). Lesions that fail this treatment or infected lesions require open drainage and secondary closure. If overlying skin is viable, open drainage can be achieved through either a single longitudinal incision or several small incisions proximally and distally(11).
Conclusion
Morel-Lavallée lesions are closed degloving-type injuries commonly associated with sports injuries caused by a shearing force, resulting in the separation of the hypodermis from the deeper fascia. Separation of the tissue planes results in a complex fluid collection with areas of fat within it. They usually occur at the thigh, pelvis, knee, gluteal region, lumbosacral area, abdominal area, and lower leg. Diagnosis includes a physical examination, MRI, and or ultrasound imaging. Conservative or minimally invasive treatment is indicated for less severe cases. However, surgical debridement might be necessary for more complex and large MLLs. If not treated in the acute or early sub-acute settings, these collections are at risk for superinfection, overlying tissue necrosis, and continued expansion.
References
- Emerg Radiol. 2014;21(1):35-43.
- British Journal of Sports Medicine - Blog. Published 2022. blogs.bmj.com/bjsm/2022/05/08/morel-lavallee-lesions-diagnosis-and-practical-management-of-these-troublesome-injuries/
- J Clin Diagn Res. Published online 2017.
- J Am Acad Orthop Surg. 2016;24(10):667-672.
- J Clin Diagn Res. Published online 2017.
- BMJ Case Rep. 2021;14(4):e243082.
- Case Rep Orthop. 2012;2012:1-5.
- J Clin Orthop Trauma. 2014;5(3):161-166.
- Journal of Sports Medicine - Blog. Published 2022. blogs.bmj.com/bjsm/2022/05/13/morel-lavallee-lesions-diagnosis-and-practical-management-of-these-troublesome-injuries-2/
- Cureus. Published online September 24, 2022.
- J Orthop. 2018;15(4):917-921.

Candice MacMillan

Latest Issue

Subscribe Today
Newsletter Sign Up
Subscriber Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up




Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue
Be at the leading edge of sports injury management
Our international team of qualified experts (see above) spend hours poring over scores of technical journals and medical papers that even the most interested professionals don't have time to read.
For 17 years, we've helped hard-working physiotherapists and sports professionals like you, overwhelmed by the vast amount of new research, bring science to their treatment. Sports Injury Bulletin is the ideal resource for practitioners too busy to cull through all the monthly journals to find meaningful and applicable studies.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Injury Bulletin brings together a worldwide panel of experts – including physiotherapists, doctors, researchers and sports scientists. Together we deliver everything you need to help your clients avoid – or recover as quickly as possible from – injuries.
We strip away the scientific jargon and deliver you easy-to-follow training exercises, nutrition tips, psychological strategies and recovery programmes and exercises in plain English.